Baseball…, what a fascinating sport! We all love throwing a baseball and playing catch, don’t we? We also admire those very, very good professional pitchers with a skilled and blazing fast pitch. Isn’t it amazing that some pitchers can throw a baseball at a speed of 100 miles per hour? How about your favorite football quarterback? Don’t you love how he throws the ball? How about watching your favorite tennis player? You may also be lucky enough to enjoy your children getting better and better at baseball…
Unfortunately, the elbow joint may suffer and get injured in various ways with the practice of throwing sports (baseball, softball, football, tennis, javelin, discus, and others). This is especially true when trying to compete at a high level, when substantial repetition is added, as well as when the throwing mechanics are poor. As a consequence, one particular ligament on the inside of the elbow, called medial collateral ligament or MCL, can tear. MCL tears will result in worse performance when throwing. Surgical reconstruction of the MCL has become widely known as the Tommy John procedure. Do you want to know why? Keep reading…!

A little bit of history
1974: a historic year for the marriage of baseball and elbow surgery. That is the year when Los Angeles Dodgers pitcher, Tommy John. sustained his MCL tear in the middle of an excellent season for the Dodgers. Most thought that Tommy John was done: he would never be able to pitch again professionally… However, he underwent elbow surgery, and went on to pitch professionally for 13 more years, winning 164 games after his surgery! His surgery, performed by Dr. Jobe, involved reconstruction of his elbow MCL with a tendon graft from his forearm; MCL reconstruction became forever known as the Tommy John procedure. Little is known of the fact that his recovery was also largely helped by Mike Marshall, a teammate with a background PhD in kinesiology, who for a whole year thought Tommy John a completely different way to pitch!

If we fast-forward to current times, the number of Tommy John procedures performed, at least in the United States, has exploded in both professional and recreational players. The question is why? It is possible that the increase in procedures is due to more injuries happening, more surgeons performing the procedure, or both. But one of the concerns expressed by some elbow experts is that our Society is pushing for it: survey studies have shown that if you ask high-school and college pitchers, their coaches, or their parents, between one third and half of them firmly believe that the Tommy John procedure will result in better velocity than before surgery, even if the ligament is actually not torn! Interestingly, studies performed in professional baseball players have shown different: about 80% will return to play at least one game, and about 70% will make it back to the major league. In other words, surgery is very good, but not universally successful. In addition, in those who return, their performance is about the same as before surgery, not better.
So,… this is the bottom line. Tears of the medial collateral ligament of the elbow do occur in throwing sports. When the MCL is torn and results in poor performance, surgical reconstruction, as performed for Tommy John, has a high chance to restore performance. But just because a thrower has elbow pain, it does not mean that the MCL is torn; the elbow joint may hurt for other reasons. In addition, many players with elbow pain when throwing will get better with the right rehabilitation program, and without surgery. The key is to consider this procedure when necessary only, and that is why evaluation by an elbow expert becomes critical.
Where is the medial collateral ligament?
The medial collateral ligament (MCL) is a relatively short and wide bundle of collagen fibers. It connects the inside aspect of the bone in the arm (humerus) to the inside aspect of one of the two bones in the forearm (ulna). The MCL is also known as ulnar collateral ligament or UCL. It contributes to keeping the elbow joint well located, and particularly resists the ulna angling away from the body. It is covered by a very powerful group of muscles (the common flexor-pronator group), and the ulnar nerve is right behind the MCL.

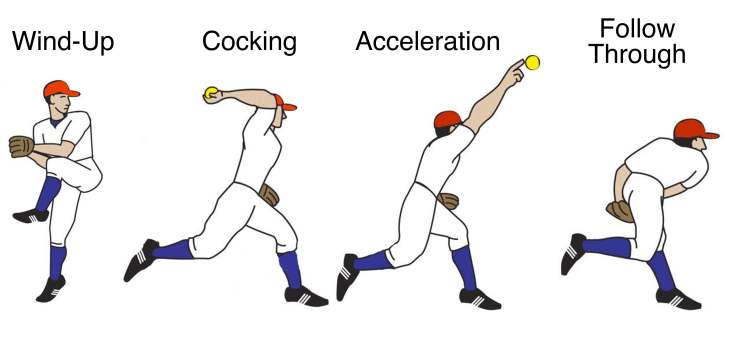
What happens to the elbow when throwing?
The mechanics of throwing have been very well analyzed, especially in baseball. The elbow gets strained the most at the transition between cocking and acceleration: as the hand is quickly placed behind, all of a sudden the pitcher uses his whole body strength to throw forward. The forearm is still heading back as the shoulder and rest of the body start to propel the ball forward, and the ligaments, muscles and tendons on the inside (medial side) of the elbow see a lot of strain. Some have calculated that the strain on the medial side of the elbow is equivalent to the strain that would be felt if a 60-pound weight was hanging off the hand (that would be like holding the weight of 5 bowling balls, as opposed to one baseball!). That is two to three times the strain that the MCL itself can tolerate before tearing. Luckily, the muscles over the location of the MCL are very strong, and protect the MCL from tearing. Otherwise, the MCL would fail in every single high-speed throw.

Why does the elbow get injured with repetitive throwing?

Tears of the MCL occur mostly because of repetitive strain. After throwing again, and again, and again… the fibers of the MCL may start to fail. The risk of fiber tearing is proportional to the number and intensity of straining cycles on the ligament. This happens with either too much pitching, pitching with poor mechanics, or both. Some risk factors have been identified: pitching over 80 times in a single game, playing competitive throwing sports all year long, and poor mechanics secondary to improper training, a lower extremity injury, poor posture, or simply fatigue. Occasionally, a player may feel a sudden pop as the MCL tearing completes all of a sudden in a single throw.
Throwing can make the elbow hurt many other ways, though. Bone spurs may develop between the ulna and the humerus as a reaction to stress, the articular cartilage may get worn out in small areas, the ulnar nerve may become irritated, or the muscles overlying the MCL may develop tendonitis or partial tears. Sometimes more than one condition coexists.
Making the diagnosis of an MCL tear

Most individuals with a symptomatic tear of the MCL only have issues when they throw. Some times, the main complaint is pain, but oftentimes is loss of performance. Your elbow surgeon will exclude other reasons for elbow pain, and confirm that the torn MCL is the culprit. The most common names you will hear when doctors describe tests to confirm an MCL tear are “milking test” and “moving valgus stress test”.
Plain radiographs are usually normal. Advanced imaging studies, such as magnetic resonance or dynamic ultrasound, may confirm the diagnosis. The elbow can be stressed under live fluoroscopy to demonstrate excessive separation between the humerus and ulna.


Treatment options
MCL tears can improve without surgery in some patients. Thus, a trial of nonoperative treatment is almost always recommended, especially in younger and recreational athletes. The program evolves in three phases: (1) complete rest from throwing (typically for 6 weeks), (2) a structured program of rehabilitation focused on throwing mechanics, including shoulder motion and strengthening, core strengthening, and strengthening of the flexor-pronator group as well, and (3) gradual return to play, with an agreement on limiting the maximum number of games and pitches for a while.
It will likely take 6 months to try to return to playing at a pretty good level with the program outlined above. Surgery is considered for those individuals that continue to have issues when throwing after completing this 6-month program, unless they are wiling to stop the practice of their throwing sport. In surgery, a portion of a tendon (tendon graft) is inserted into bone tunnels drilled in the humerus and ulna along the course of the MCL. Most of the times, the tendon graft is obtained from the patient’s forearm or leg (autograft), but occasionally tendon from a donor is used (allograft). After surgery, the elbow is immobilized briefly and therapy starts with a program similar to the one outlined above. Most patients return to competitive playing one year after surgery, and most state that they do not perform at their highest level for a whole other year. Two years to be your best again!
A few final words…
So many individuals are developing MCL tears due to poor mechanics or excessive throwing! Our society needs to make some efforts to improve training and advice players, coaches and parents about the safe limits of throwing. It is also important to consider surgery only if (1) the MCL is confirmed to be the culprit of poor performance, and (2) a well-structured 6 month program of therapy has failed to allow the patient to return to play.
Reconstruction of the MCL does allow 70 to 80 percent of individuals to return to play, likely at the same level…, but it may take up to two years, and a very good therapy program focused on the mechanics of throwing is paramount. Hopefully, many excellent sport players can be helped by MCL reconstructions and replicate to some extent the outstanding career of the legendary Tommy John!