The human body is a masterpiece of engineering design! The ability to use our hands is extremely important for the majority of our daily activities. Proper use of the hands for various tasks requires being able to position the hands out in space and move them back closer to our body. Good movement of the elbow joint is paramount for hand positioning in space. Unfortunately, the elbow is particularly prone to stiffness after injury or surgery, or as a consequence of certain diseases such as osteoarthritis and rheumatoid arthritis. Those of you that cannot move your elbows fully will know how limiting elbow stiffness can be!

Movements of the elbow joint
Three bones meet at the elbow joint: the humerus (the bone in the arm) and the radius and ulna (the two bones in the forearm). The main movements of the elbow are flexion and extension. The elbow behaves like a complicated hinge. The radius and ulna move together relative to the humerus to straighten (extension) or bend (flexion) the joint. The elbow also participates in forearm rotation. The ability to place the hand palm up, palm down, or every position in between, depends on the radius rotating around the ulna. Forearm rotation requires movement of the radial head at the elbow and the lower end of the radius at the wrist.

Joint motion is measured in degrees. When the elbow is fully straight, extension is considered to be zero degrees. Most healthy individuals can bend their elbow to 140 degrees or more. Very flexible individuals may be able to straighten their elbows beyond zero degrees (this is called hyperextension) and bend the elbow so that their forearm rests on the arm fully. Forearm rotation may be measured using the thumbs or a pen held with the fist closed. Most individuals can place the palm up so that the thumb is almost parallel to the floor (75 to 85 degrees of supination); the same is true for placing the palm down (75 to 85 degrees of pronation).

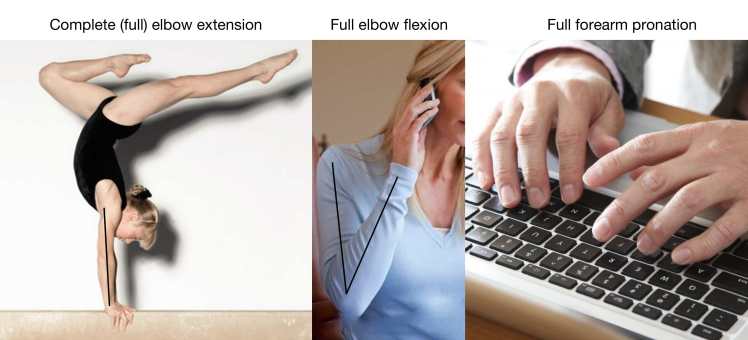
Luckily, not every activity we perform requires placing the elbow fully straight or fully bent. The range of degrees of motion that is required for most common activities has been analyzed carefully. It turns out that individuals who can extend their elbow to at least 30 degrees, bend their elbow to 130 degrees, and rotate their forearm approximately 50 degrees in each direction seem to be able to perform most of their desired activities. Individuals who are able to move at least this much are considered to have a functional arc of motion. Obviously, certain occupations do require normal motion; for example, gymnasts need to lock their elbows completely straight for many of their pirouettes.




We would all agree that increasing use of modern technology has had a substantial impact in our lives. We use computers constantly, and smartphones all the time for communication and social networking. You may be reading this blog on your iPhone or Google phone right now! Interestingly, incorporation of technology in our lives has impacted the needs for the elbow too! Use of computer keyboards becomes cumbersome if pronation is limited. If you try to talk on a cellphone and your elbow bending is limited, you may need to turn the neck too much and eventually get neck pain when you are on the phone.
Substantial loss of elbow motion has a tremendous negative impact in our lives. The shoulder, hand and neck cannot compensate for loss of elbow motion, and simple activities such as getting dressed, eating, driving, using a computer, reaching out for objects, or using the affected hand for personal hygiene may be impossible. No wonder individuals with severe elbow stiffness are wiling to undergo surgery so that their motion improves!
Why is the elbow so prone to stiffness?

Elbow specialists know well that the elbow joint becomes stiff more often than other joints. Loss of elbow motion occurs typically as a consequence of injuries or after elbow surgery. Like any other joint, the elbow is enclosed inside a capsule -like a bag- made mostly of collagen, the main fiber component of the skeleton. If the capsule becomes less elastic, too thick, or gets stuck to the adjacent bones, it does not stretch enough to allow full motion. This excessive capsular fibrosis is present to some extent in almost all stiff elbows. The capsule in the front will limit straightening the elbow, whereas the capsule in the back will limit how much the elbow can be bent. For reasons that are not completely clear, the elbow is particularly prone to heal after injuries or surgery laying down too much scar tissue in the capsule.
Complete elbow motion also requires that the ends of the bones fit into each other. For example, when the elbow is fully straight, the back of the ulna (olecranon) fits into a cavity in the back of the humerus (olecranon fossa). When the elbow is fully bent, the radial head and the front of the ulna (coronoid) need to fit into the front of the humerus (into the radial head and coronoid fossae). Deformity after fracture, or formation of bone spurs at the end of the bones or inside the fossae, will thus block motion.

Another mystery around the elbow joint has to do with formation of bone outside of the skeleton, known as heterotopic (or ectopic) ossification. In some individuals, extra bone forms in the substance of the soft-tissues (capsule and ligaments or muscle), some times to the point of creating a true bridge of bone between the elbow bones, which will limit or even completely block motion. Heterotopic ossification can form after injuries, but it can also occur in individuals that have suffered severe burns or an injury to the brain or spinal cord.

Why some people form excessive scar tissue, bone spurs and even heterotopic bone in the elbow, whereas others won’t, continues to be a matter of debate. The exact same injury or surgery will end with pretty good motion in some individuals and really poor motion in others. This variability amongst individuals is likely due at least in part to the fact that we are all different: some have blue eyes and blonde hair, some green eyes and dark hair,… some suffer stiffness after injury or surgery, and some don’t!
If your forearm rotation is limited, things can be more complicated. Normal forearm rotation requires a normal elbow, forearm and wrist. Elbow problems may lead to loss of pronation and supination, but not uncommonly, the forearm and the wrist are involved as well. This makes restoration of forearm rotation with surgery a bit more complicated in most instances.
Can elbow stiffness be prevented?
To some extent, yes. Injuries and surgery both trigger a healing response. The intensity of the healing response is part of the reason why some elbows will become more stiff. The key elements of prevention include (1) modulating the healing response, and (2) starting motion exercises as soon as possible.
If you had an elbow injury or have undergone surgery, the most important thing you can do to prevent stiffness is to follow the instructions of your elbow specialist. Even though starting motion soon helps, it may not be safe right away depending on the nature of your injury or surgery. Once allowed, practice gentle motion of your elbow joint in all for planes discussed above (flexion, extension, pronation and supination). In addition, keeping inflammation under control helps too. This can be achieved by wrapping the elbow with a compressive dressing or sleeve, keeping it elevated above the level of your heart when sitting or lying down, application of ice or cold several times a day (especially over the first few days), and anti-inflammatory medications if authorized by your elbow specialist. Sometimes further motion may be achieved with use of braces or motion machines to stretch the elbow.
If my elbow is permanently stiff, is it possible to restore elbow motion surgically?
If you have permanent limitation of elbow motion, an elbow specialist may be able to help you. Most of the times, elbow motion can be improved surgically, although restoring motion to completely normal is very, very difficult. If your motion arc is within the functional range, you may be recommended not to try surgery, because you are so close to normal. But if your motion is very limited, you will be happy to see it improved, even if you do not get complete extension, flexion, pronation or supination.
Provided the joint surfaces are not badly damaged, elbow replacement does not need to be considered. Surgery typically involves removal of excessive scar tissue, removal of the thickened, non-elastic capsule, and removal of all bone spurs, areas of bone deformity, and ectopic bone that get in the way of motion. Technical names you may hear when elbow surgeons discuss the details of surgery include elbow debridement, contracture release, arthrolysis, or osteocapsular arthroplasty…, wow! They all mean the same: the surgeon removes soft-tissues and bone spurs or pieces in a safe and sequential fashion until complete motion is restored. And believe it or not, these procedures are very commonly performed nowadays arthroscopically: small skin cuts are used to perform the surgery while visualizing with a camera introduced in the joint.
You are probably already thinking how important it must be to move the elbow right after surgery so that it does not freeze up again! Depending on the nature of your surgery, this may be accomplished with self-performed exercises, the help of a physical therapist, braces, or a continuous passive motion machine. Keeping inflammation under control as described above is important too. Rarely, if you had lots of heterotopic bone removed, one dose of radiation may be recommended. Whatever it takes to be able to move your elbow again!
2 thoughts on “Did you know that the elbow joint is particularly at risk for stiffness?”
Comments are closed.